Plastic Surgery Perspective
Breast Reconstruction for
Gene-Susceptible Patients
A comprehensive guide to nipple-sparing mastectomy, modern reconstruction techniques, and sensory restoration for BRCA, CHEK2, and other hereditary breast cancer gene carriers.
www.chaiyasate-plasticsurgery.comMeet the Surgeon
Dr. Kongkrit Chaiyasate
Double Board Certified Plastic & Reconstructive Surgeon
Dr. Kongkrit Chaiyasate is an internationally recognized microsurgeon and fellowship-trained specialist in advanced breast and body reconstructive surgery. With over 3,500 DIEP flap reconstructions performed, he is one of the most experienced microsurgeons in the field.
His expertise spans the full spectrum of breast reconstruction for gene carriers — from nipple-sparing mastectomy with direct-to-implant reconstruction to complex autologous DIEP flap procedures with Resensation neurotization.
3,500+
DIEP Flap Reconstructions
Fellowship
Trained Microsurgeon
Double
Board Certified
International
Recognition & Practice


Dr. Chaiyasate in the operating room at Corewell Health William Beaumont with advanced microsurgical equipment

Dr. Chaiyasate performing microsurgery with high-powered surgical loupes and headlight
Gene Risk Stratification
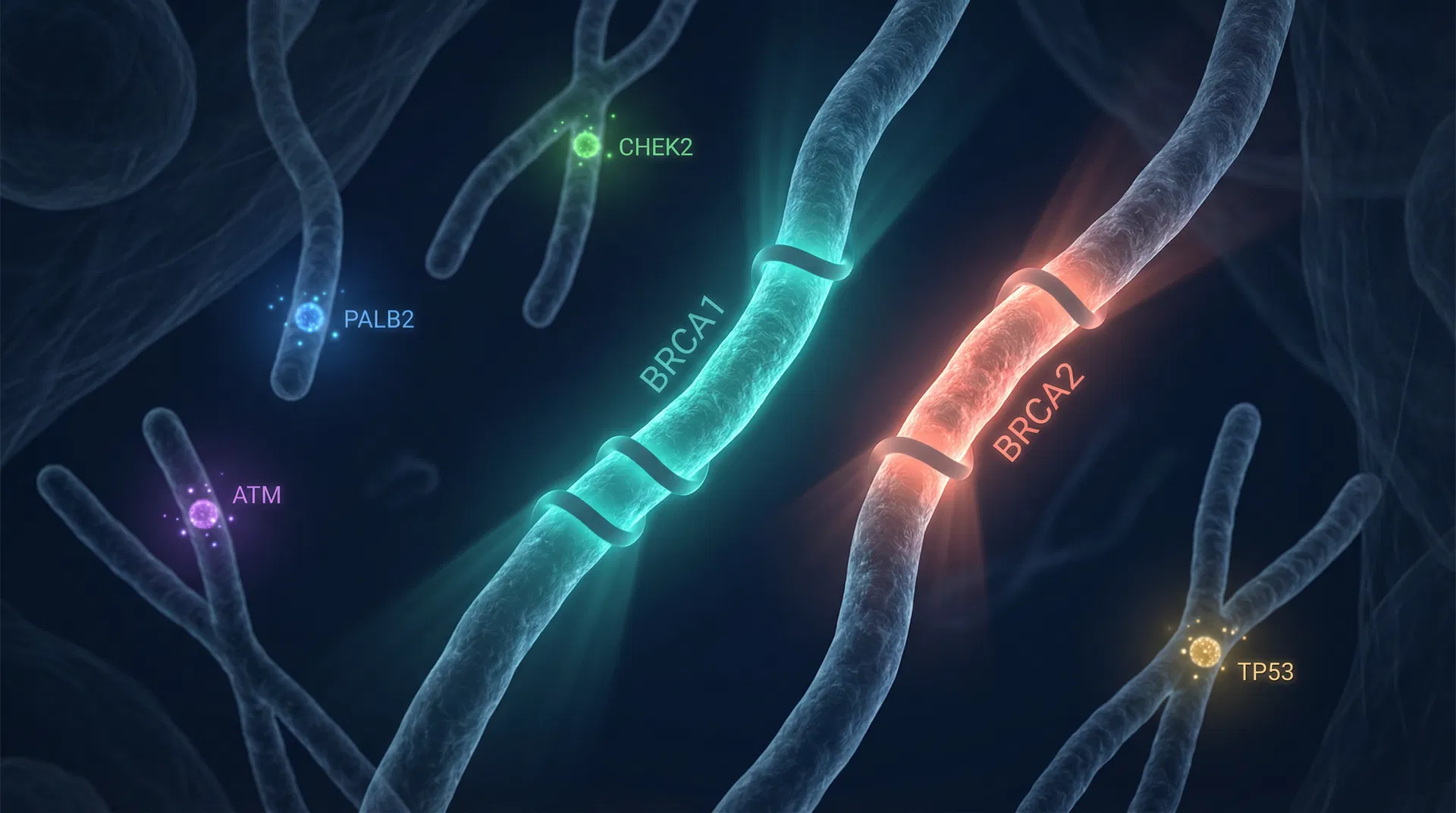
Understanding Hereditary Breast Cancer Genes
Pathogenic variants in breast cancer susceptibility genes significantly increase lifetime risk. High-penetrance genes (BRCA1, BRCA2, TP53, PTEN, CDH1) confer a greater than 4-fold increased risk, while moderate-penetrance genes (CHEK2, ATM, PALB2) confer a 2- to 4-fold increased risk.
The plastic surgery approach must be tailored based on the specific gene mutation, penetrance level, radiation safety profile, and the patient's individual risk-benefit assessment for risk-reducing mastectomy (RRM).
| Gene | Penetrance | Lifetime Risk | CBC Risk | RRM | Radiation | Notes |
|---|---|---|---|---|---|---|
| BRCA1 | High | 55–72% | 40–60% | Recommended | Safe | Highest CBC risk, especially young onset |
| BRCA2 | High | 45–69% | 26–40% | Recommended | Safe | Moderate CBC risk |
| TP53 | High | Very High | High | Recommended | Contraindicated | Li-Fraumeni syndrome; avoid RT |
| PTEN | High | 25–50% | Moderate | Discuss | Safe | Cowden syndrome |
| CDH1 | High | 39–52% | Moderate | Discuss | Safe | Lobular cancer risk |
| PALB2 | Mod–High | 35–60% | Emerging | Case-by-case | Safe | Emerging high-risk data |
| CHEK2 | Moderate | 25–30% | Moderate | Not routine | Safe | 1100delC most studied variant |
| ATM | Moderate | 25–30% | Moderate | Not routine | Safe | Limited toxicity data |
| STK11 | High | 32–54% | Moderate | Discuss | Safe | Peutz-Jeghers syndrome |
| RAD51C/D | Moderate | Emerging | Emerging | Not routine | Safe | Limited data |
Sources: ASCO/ASTRO/SSO Guidelines (Tung et al., JCO 2020); NCCN Guidelines v2.2025
Nipple-Sparing Mastectomy
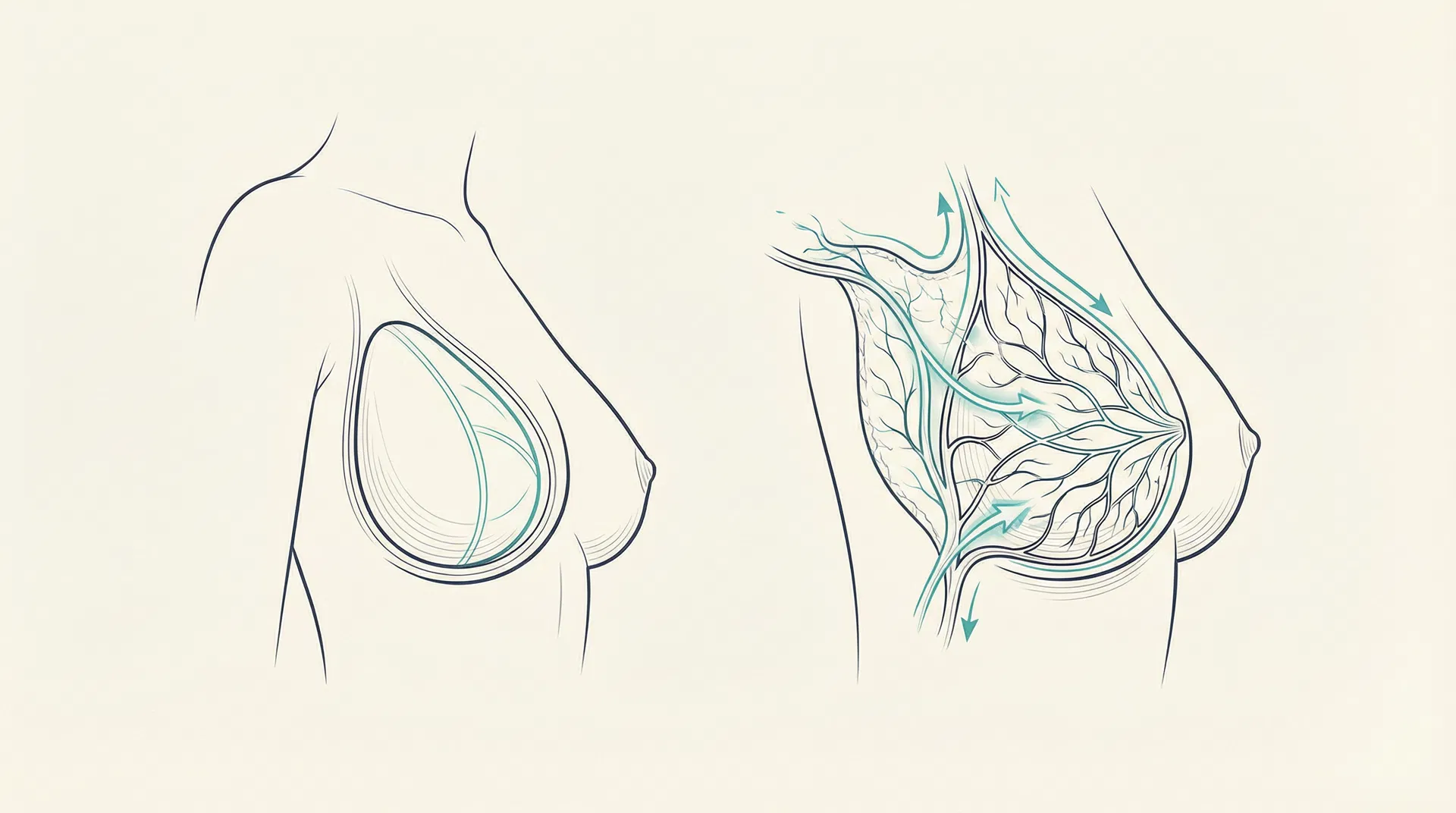
The Gold Standard: Nipple-Sparing Mastectomy
Nipple-Sparing Mastectomy (NSM) preserves the entire skin envelope including the nipple-areolar complex (NAC) while removing all breast parenchyma. For gene carriers undergoing prophylactic surgery, NSM has become the preferred approach, offering 90–95% risk reduction with superior aesthetic outcomes.
"NSM is reasonable for both therapeutic and contralateral risk-reducing mastectomy in BRCA1/2 carriers."
— ASCO/ASTRO/SSO Guidelines, JCO 2020
Oncologic Safety
Multi-institutional studies confirm local recurrence rates comparable to total mastectomy. Risk reduction of 90–95% is maintained in BRCA carriers (JAMA Surgery, 2018).
Incision Approaches
Inframammary fold (IMF) incision is most common and offers the best cosmesis. Lateral radial, periareolar, and Wise pattern incisions are alternatives based on anatomy.
Ideal Candidacy
Prophylactic mastectomy patients are ideal candidates. Tumor must be >2cm from nipple, no clinical nipple involvement, no inflammatory breast cancer, and adequate skin flap perfusion.
Direct-to-Implant Reconstruction
Direct-to-Implant Reconstruction
Direct-to-Implant (DTI) reconstruction places the permanent implant at the time of mastectomy, eliminating the need for a tissue expander phase. Prepectoral placement (above the pectoralis major muscle) is preferred for prophylactic cases, using acellular dermal matrix (ADM) for implant coverage and support.
Complication Rates
Higher risk with larger specimens, age >50, radiation history
DIEP Flap Reconstruction
DIEP Flap: Autologous Reconstruction
The Deep Inferior Epigastric Perforator (DIEP) flap is the gold standard for autologous breast reconstruction. It transfers skin and fat from the lower abdomen via microsurgical free tissue transfer, preserving the rectus abdominis muscle (unlike the older TRAM flap). For gene carriers, DIEP offers a lifetime reconstruction without implant-related concerns.
Advantages for Gene Carriers
- ◆Natural tissue — no implant-related complications or replacements
- ◆Higher long-term satisfaction (BREAST-Q data)
- ◆No capsular contracture risk
- ◆Can be combined with neurotization for sensation
- ◆Ideal for bilateral reconstruction in prophylactic cases
- ◆Can reconstruct to desired smaller size for large-breasted patients
Outcomes Data
in experienced centers
adjusted mean difference vs implant (BREAST-Q)
adjusted mean difference vs implant
Source: Broyles et al., Systematic Review, 2022 (121,302 patients)
Resensation & Neurotization
Restoring Feeling
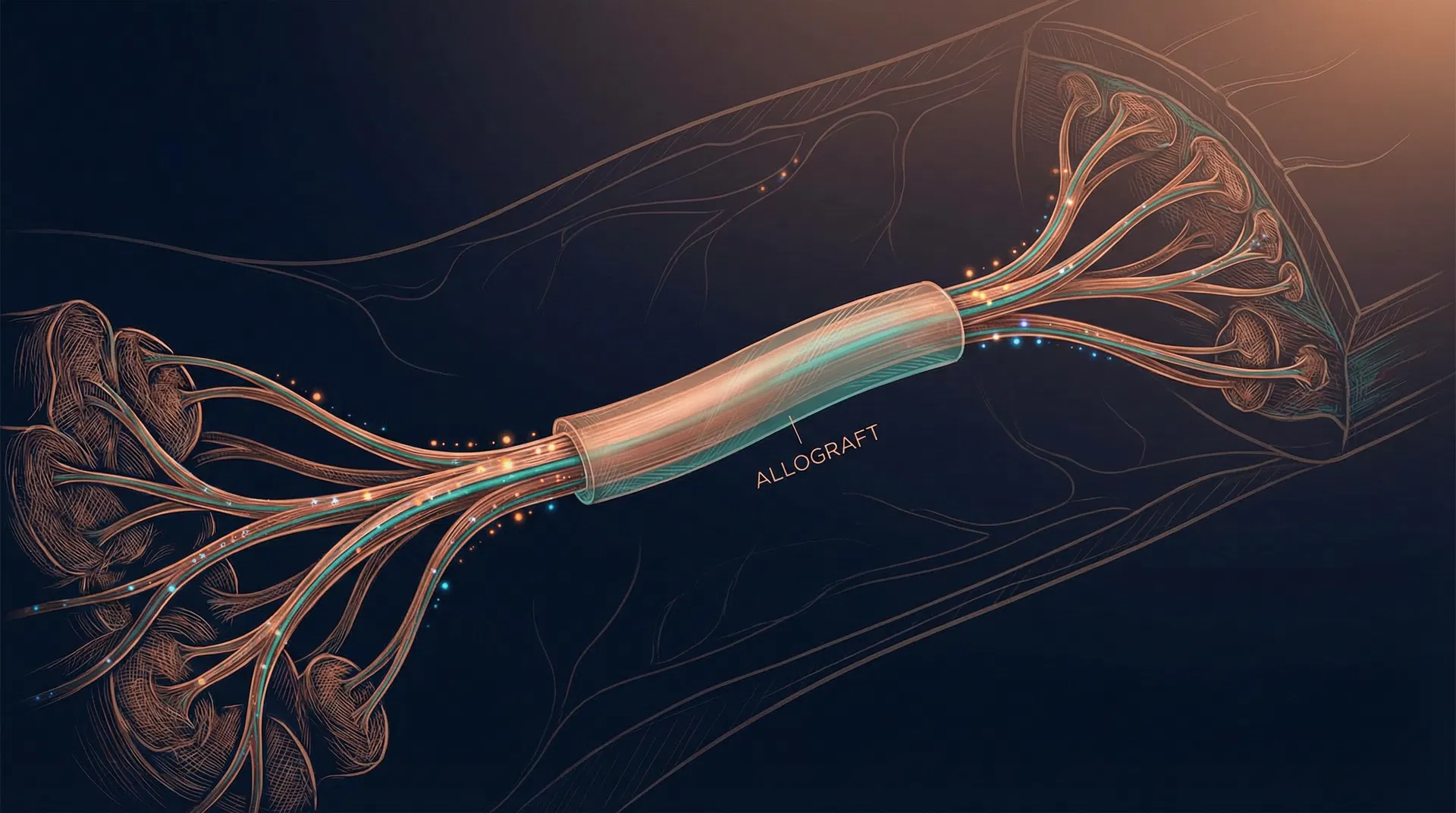
Resensation: Breast Neurotization
Resensation is a surgical technique of breast neurotization (nerve repair) performed during reconstruction. It uses a processed nerve allograft (Avance, by Axogen) to bridge the gap between chest wall intercostal nerves and the reconstructed breast tissue or NAC.
The procedure adds approximately 15–30 minutes to operative time and can be performed with both implant-based (DTI) and autologous (DIEP flap) reconstruction.
Key Outcomes (Peled et al., 2023)
Neurotization with DIEP Flap
The sensory nerve of the DIEP flap (branch of T10–T12 intercostal nerve) is identified within the flap and coapted end-to-end or end-to-side to the recipient intercostal nerve (T3–T5) at the chest wall. Nerve allograft can bridge the gap if needed.
- ◆ Innervated DIEP flaps show improved postoperative sensibility (Bubberman et al., 2024 RCT)
- ◆ Superior sensation outcomes regardless of flap type (Tajziehchi et al., 2024)
- ◆ Better psychosocial and sexual well-being reported (Shyu et al., 2025)
Large & Ptotic Breasts
Managing Large & Ptotic Breasts
Patients with macromastia and severe ptosis were historically considered poor candidates for NSM due to significantly higher rates of nipple-areolar complex (NAC) necrosis, aesthetic failures, and difficulty ensuring complete glandular removal. Modern techniques now allow these patients to safely undergo nipple-sparing procedures.
Ischemic Complications
Long skin flaps and excessive tension on the NAC drastically increase the risk of partial or complete nipple necrosis and skin flap ischemia.
Aesthetic Failures
A redundant, oversized skin envelope cannot be adequately filled by an implant without causing unnatural folding, wrinkling, and "bottoming out."
Oncologic Access
Technically difficult to ensure complete glandular removal at the far periphery of a very large breast through a cosmetically acceptable incision.
Option A: Staged Breast Reduction (Nipple Delay)
Stage 1: Reduction
- ■Standard oncoplastic breast reduction or mastopexy
- ■Lifts NAC to ideal anatomical position
- ■Divides deep perforating vessels to the nipple
- ■Establishes subdermal blood supply
The Delay Period
- ■3–6 months waiting period
- ■Allows robust revascularization of the NAC
- ■Blood supply shifts to subdermal plexus
- ■Scars mature and soften
Stage 2: NSM + Recon
- ■Definitive Nipple-Sparing Mastectomy
- ■Incision through previous reduction scars
- ■Immediate DTI or DIEP flap reconstruction
- ■Neurotization (Resensation) performed
Clinical Impact: This staged approach reduces NAC necrosis rates from >20% down to <3%, while achieving a lifted, smaller, more youthful breast.
Option B: Single-Stage Skin-Reducing NSM (Wise Pattern)
For patients who prefer to avoid multiple surgeries, the single-stage skin-reducing NSM uses a Wise pattern (inverted-T) incision to simultaneously perform mastectomy, skin envelope reduction, and immediate reconstruction. The excess inferior skin is de-epithelialized to create an inferior dermal flap that provides robust lower pole support.
✓ Advantages
- ◆ Single operation — oncologic risk reduction + aesthetic reconstruction
- ◆ Immediate breast lift and volume reduction
- ◆ Dermal flap acts as autologous sling, reducing need for ADM
⚠ Considerations
- ◆ Higher NAC ischemia risk vs. staged approach
- ◆ Best for non-smokers with controlled BMI and moderate ptosis
- ◆ Requires meticulous flap design for adequate NAC perfusion
Reconstruction Algorithm
Reconstruction Algorithm for Gene Carriers
The choice of reconstruction pathway depends on breast size, degree of ptosis, patient preference, body habitus, and the desire to avoid implants. All pathways now incorporate Resensation (neurotization) as a universal standard.
Standard / Small-to-Moderate Breasts
Or: NSM → DIEP Flap (innervated) + Resensation
Large / Ptotic Breasts — Staged
Large / Ptotic Breasts — Single Stage
Patients Requiring Radiation
TP53 carriers: Radiation CONTRAINDICATED — mastectomy only
Universal Standard
All pathways incorporate Resensation (Neurotization)
Restoring sensory function is now a critical component of every reconstruction pathway, improving quality of life, eliminating chronic pain, and enhancing psychosocial well-being.
Gene Risk Calculator
Personalized Risk Assessment
Select your gene mutation and provide basic information to see your estimated risk profile, recommended screening, surgical options, and personalized reconstruction pathway.
For educational purposes only — consult your physician for personalized medical advice
Patient FAQ
Patient Stories
After testing positive for BRCA1, I was terrified. Dr. Chaiyasate walked me through every option and helped me understand that prophylactic surgery didn't mean losing who I am. The DIEP flap with Resensation gave me breasts that look and feel natural. I can actually feel my children hug me.
Sarah M., age 38
BRCA1 carrier, bilateral DIEP flap with Resensation
As a CHEK2 carrier with large breasts, I was told by other surgeons that nipple-sparing wasn't possible for me. Dr. Chaiyasate performed a staged breast reduction first, then the mastectomy with direct-to-implant reconstruction. The results exceeded my expectations.
Jennifer L., age 45
CHEK2 carrier, staged reduction + NSM + DTI
The Resensation procedure was a game-changer for me. I had prepared myself to never feel anything again, but within 6 months I started getting sensation back. By a year, it was remarkable. I wish more women knew this was possible.
Michelle R., age 42
BRCA2 carrier, NSM + DTI + Resensation
Schedule a Consultation
Request a Consultation
Take the first step toward proactive breast health. Dr. Chaiyasate and his team are here to guide you through your options with compassion and expertise.
Office Location
36800 Woodward Ave, Suite 112
Bloomfield Hills, Michigan 48304
Phone
(947) 274-8300Consultation Request Form
Key References
- Tung NM, et al. Management of Hereditary Breast Cancer: ASCO, ASTRO, and SSO Guideline. J Clin Oncol. 2020;38(18):2080-2106.
- Peled AW, et al. Outcomes after neurotization of the nipple-areola complex in nipple-sparing mastectomy. Plast Reconstr Surg. 2023.
- Broyles JM, et al. Implant-based vs autologous reconstruction: Systematic review. JAMA Surg. 2022.
- Bubberman JM, et al. Innervated DIEP flap: Randomized controlled trial. 2024.
- Salibian AA, et al. Staged breast reduction before NSM. Ann Breast Surg. 2019.
- Friedman HI, et al. Skin-reducing NSM with prepectoral DTI. Plast Reconstr Surg. 2019.
- Reitsamer R, et al. Prepectoral DTI after NSM: 200 breasts. 2019.
- Jagasia P, et al. ABR with neurotization: Meta-analysis. 2025.
- Shyu S, et al. Neurotized breast patients: Psychosocial and sexual well-being. 2025.
- NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. v2.2025.